When ADHD and Acquired Brain Injury Meet: Rethinking Communication Rehabilitation
In February 2026, I was invited to speak at Acquired Brain Injury Clinical Excellence Network (ABICEN)’s conference for Speech and Language Therapists (SLTs) in acquired brain injury services: “Navigating the cognitive communication crossroads of brain injury and neurodivergence.”
My talk focused on working with adults with ADHD in acquired brain injury (ABI) services, drawing on my combined experience as an adult neuro Speech and Language Therapist and Communication Coach supporting neurodivergent clients, particularly adults with ADHD and/or autism.
This feels like an important conversation to share more widely. SLTs working in ABI services are very likely to have adults with ADHD on their caseloads, whether diagnosed, suspected or previously unrecognised. ADHD does not sit neatly outside ABI rehabilitation. For many clients, it may already be part of the clinical picture, shaping communication, engagement, emotional responses, carryover and outcomes.
This article offers an overview of why ADHD matters in ABI rehabilitation, how it can overlap with cognitive-communication profiles, and how we might begin to adapt our clinical thinking and practice.
For SLTs and rehabilitation professionals who would like to explore the topic in more depth, an extended 80-minute recorded webinar and slides are available for purchase at the end of this article.
Why ADHD matters in ABI services
ADHD and acquired brain injury are not mutually exclusive.
In a Canadian adult sample, Ilie et al. (2015) found that adults with a history of traumatic brain injury were 2.64 times more likely to report an ADHD diagnosis than those without traumatic brain injury. This does not prove a simple cause-and-effect relationship, but it highlights an important clinical overlap for ABI services.
There are a few possible reasons this matters.
Some ADHD traits, such as impulsivity, risk-taking behaviour and impaired attention, may increase the likelihood of accidents or injuries.
At the same time, some adults may have had ADHD traits long before their injury, but developed complex ways of coping, compensating or masking.
After ABI, those coping strategies may no longer be sustainable.
Someone who previously relied on last-minute urgency, over-preparation, anxiety-driven performance, complex systems or high levels of self-monitoring may suddenly find that the same scaffold no longer holds.
After ABI, ADHD coping strategies that appeared previously effective may no longer be sustainable.
For Speech and Language Therapists, this matters because ADHD can affect communication, rehabilitation engagement, formulation, goal-setting and carryover.
It can also change how we interpret what we are seeing.
What appears to be inconsistent engagement, reduced insight, poor carryover or lack of motivation may sometimes have a very different explanation.
Overlapping communication profiles - ADHD vs. Cognitive Communication Disorder (CCD)
ADHD-related communication patterns can overlap significantly with acquired cognitive-communication difficulties post brain-injury.
This might include difficulties with:
turn-taking and conversational flow
discourse organisation
attention and monitoring
working memory during conversation
self-monitoring and repair
word-finding or disorganised output
social cognition and pragmatics
emotional regulation within interactions
variability across contexts
This overlap can make our formulation as Speech and Language Therapists more complex.
Is the communication difficulty primarily due to the brain injury?
Is it linked to longstanding ADHD?
Is it affected by fatigue, anxiety, sensory load, pain, medication timing, low self-belief or the demands of the environment?
Or is it the interaction between several of these?
In practice, the most useful question may not always be:
“Which diagnosis explains this?”
It may be:
What might be driving these communication patterns?
When ADHD and ABI overlap, communication can become difficult to formulate because the same outward behaviour may have several possible drivers.
For example, a client who interrupts frequently might be experiencing reduced inhibition, difficulty holding a thought in working memory, anxiety, reduced awareness of turn-taking cues, or pressure to keep the conversation engaging.
A client who appears disengaged might be fatigued, under-aroused, overwhelmed, ashamed, avoidant, or struggling to connect the task to something meaningful.
The behaviour may look familiar from ABI rehabilitation, but the underlying mechanism may not be the same.
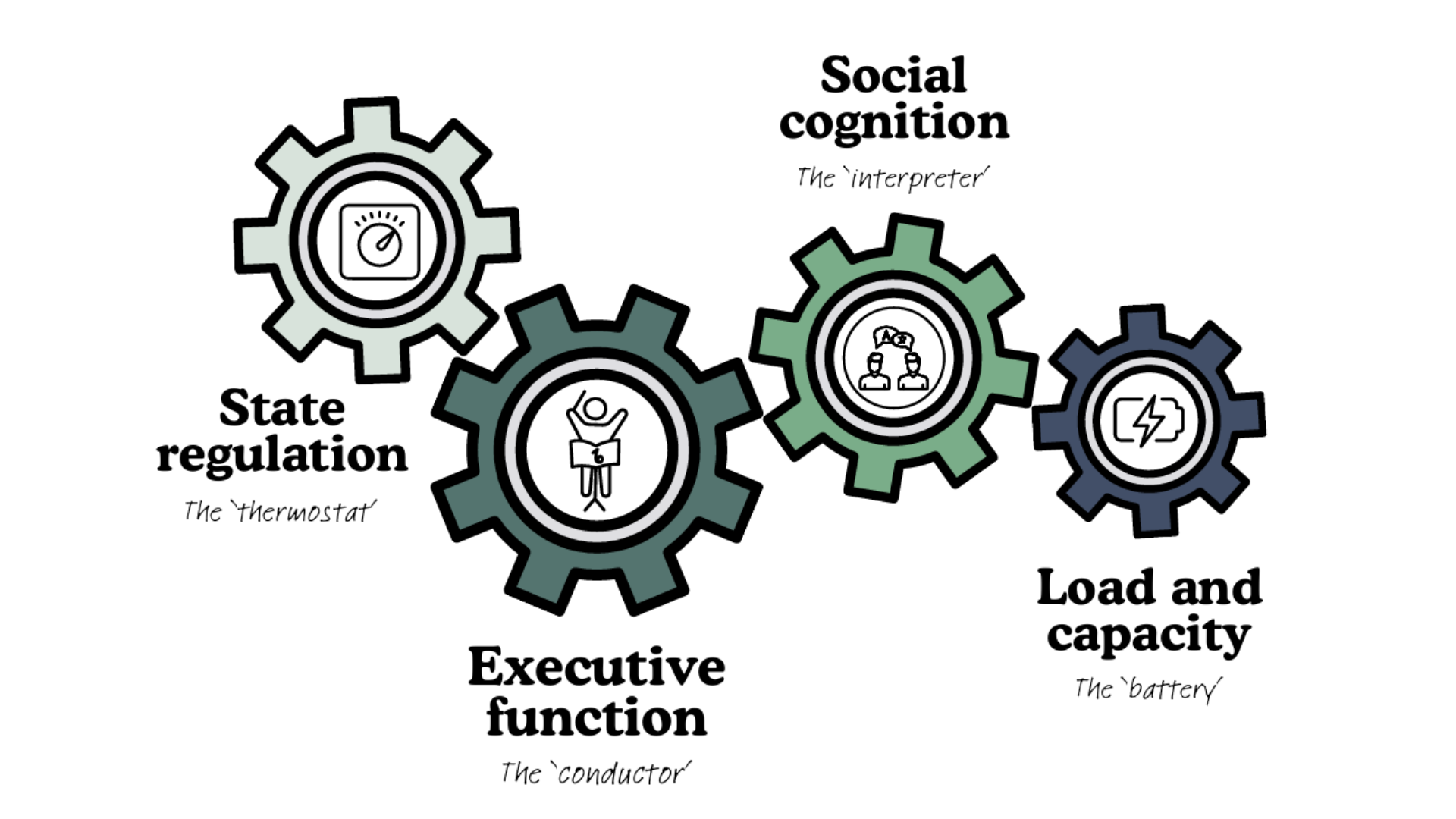
ADHD-related communication patterns may be driven by several interacting factors, including executive function, social cognition/pragmatics, state regulation and load/capacity.
The image above is how I have started to hold this in mind clinically.
As ABI clinicians, we are already used to thinking about executive function, social cognition, cognitive load and fatigue. These are central to cognitive-communication rehabilitation, and they remain highly relevant when ADHD is part of the picture.
Executive function differences may affect working memory, inhibition, planning, attention regulation, self-monitoring and repair. In real conversations, that might mean losing the thread, speaking before planning, struggling to wait for a turn, missing details, or finding it difficult to notice and repair a communication breakdown.
Social cognition and pragmatics include how someone reads the interaction, understands the other person’s perspective, picks up on tone or implied meaning, manages turn-taking, and adapts communication to the context.
Again, none of this is unfamiliar territory for ABI SLTs.
However, ADHD adds another layer.
ADHD has often been understood through the lens of executive function challenges, but that does not fully explain the variability many people describe.
State regulation accounts of ADHD draw attention to arousal and activation - essentially, whether the person’s nervous system is in a state that supports thinking, engagement and communication.
This helps explain why someone may communicate clearly in one context, then struggle to access the same skills in another. Their communication may shift depending on interest, urgency, perceived pressure, emotional state, sensory load, fatigue, or how safe and understood they feel in the interaction.
This is not unique to ADHD. We see variability, fatigue effects and reduced capacity in many ABI presentations too.
The difference is that, when ADHD is also part of the picture, these patterns may be longstanding, more interest- or urgency-driven, and more closely linked to neurodivergent regulation, motivation and threat responses.
In our clinical formulation, rather than trying to neatly separate ADHD from ABI communication symptoms, we can use both lenses to build a fuller picture.
The question becomes “What is making communication harder here - and what might reduce the load?”
Why ABI SLTs are well placed to support clients with ADHD
I believe ABI SLTs should feel encouraged that they already have many of the skills needed to support adults with ADHD-related communication difficulties.
We already understand cognitive-communication rehabilitation.
We already work with:
executive functioning
metacognitive strategy training
external aids
functional communication practice
social cognition and pragmatics
communication partner training
participation goals
environmental adaptations
generalisation and carryover
These are highly transferable.
We can support people to externalise executive functions, reduce reliance on working memory, practise strategies in real contexts, support carryover, and adapt the environment so communication is less dependent on effort alone.
We are also used to thinking systemically. We know that communication does not happen inside one person. It happens between people, in real environments, with real pressures, histories and relationships.
What we may need to do differently when ADHD is part of the picture
The conditions around therapy
Although ABI SLTs are well placed to support adults with ADHD-related communication difficulties, we may need to pay closer attention to the conditions around therapy - keeping in mind how ADHD may impact engagement and the therapeutic relationship.
This includes how we offer feedback, how we frame strategies, how much autonomy the client experiences, and whether the work reduces load or adds to it.
Many neurodivergent adults have a long history of being misunderstood, corrected, criticised or judged for the way they communicate. Over time, this can create shame, self-doubt and a sense of always having to monitor or explain themselves. After ABI, there may also be an additional loss of confidence, identity and cognitive capacity. That history can shape how assessment, feedback, goal-setting and home practice are experienced.
This is where neurodiversity-affirming and trauma-informed practice becomes particularly important.
Threat responses - rejection sensitivity and demand avoidance
Neurodivergence can also be frequently associated with threat-driven nervous system responses that shape communication and therapy engagement.
These patterns matter not only in the therapy room, but in the client’s everyday interactions too. Feedback, disagreement, advice, expectations, requests and perceived criticism may all affect how safe, regulated and able to communicate someone feels.
One example of this is rejection sensitivity, sometimes described as Rejection Sensitive Dysphoria (RSD), which many adults with ADHD describe as a strong emotional and physiological response to real, perceived or anticipated criticism, rejection or social evaluation.
This is clinically relevant because feedback is generally built into rehabilitation. A well-intended SLT’s suggestion may land as shame, failure or contribute to a client’s internal monologue that they are “getting it wrong yet again”. What we might see in their behaviour is over-apologising, over-explaining, defensiveness, shutting down, avoidance, people-pleasing or rumination afterwards.
We do not need to avoid feedback, but we may need to offer it with more care: asking permission, explaining our intention, balancing challenge with strengths, and keeping the therapeutic relationship front-and-centre.
Another nervous system response frequently experienced in neurodivergent clients is demand avoidance, which for some people may be defined as ‘PDA’. PDA has historically stood for Pathological Demand Avoidance, although many people prefer Persistent Drive for Autonomy because it places more emphasis on autonomy and threat rather than “defiance”.
In therapy, demands can be everywhere - but may not always be obvious to us as clinicians. A demand might be a homework task, a therapy goal, an outcome measure, a piece of advice, a suggested strategy, a report recommendation, or even the expectation to engage in a particular way during the session.
For some neurodivergent clients, especially when capacity is already reduced after ABI, perceived pressure or loss of control may trigger a threat response. This may show up as avoiding tasks, agreeing in the session but not following through, negotiating, deflecting with humour, becoming irritated, shutting down, or resisting suggestions that appear clinically reasonable.
If we only interpret these behaviours as poor motivation or non-compliance, we may miss what is happening underneath.
Clinically, this means paying close attention to autonomy, pacing and collaboration. Strategies may need to be offered as experiments rather than instructions. Home practice may need to feel genuinely chosen, relevant and manageable.
Masking and the cost of “better” communication
We also need to be careful that communication therapy does not accidentally encourage masking.
A client may appear to communicate “better”, including on our standardised assessment tools, because our intervention is encouraging them to communicate in a more ‘neurotypical’ way. But internally this may rely on using high levels of effort, anxiety and self-monitoring.
This is particularly relevant when working on conversation strategies, social communication, turn-taking, pacing, repair or workplace communication.
Our aim should not be to ‘make the person appear more neurotypical’. It is to support communication that is effective, authentic, sustainable and aligned with the person’s own goals, strengths and values.
This is why goal-setting needs to be values-aligned, strengths-focused, person-centred and functional.
Therapeutic strategies should reduce load where possible, not simply ask the person to work harder to appear more acceptable to others.
Supporting engagement in an ADHD nervous system
ADHD may shape engagement through interest, novelty and urgency.
Many adults with ADHD describe finding it easier to engage when something feels meaningful, immediate, novel or emotionally salient. Future rewards, abstract goals or delayed outcomes may not create the same level of activation.
In rehabilitation, this has practical implications. Home practice may be more accessible when it is brief, relevant, varied and linked to a clear immediate purpose. Feedback may need to be timely. Progress may need to be visible. Tasks may need to connect with something the person genuinely cares about.
At the same time, many adults with ADHD have learned to rely on urgency, pressure or hyperfocus to get things done. After ABI, that can carry a much higher fatigue cost. Urgency and hyperfocus may support short-term performance, but they can also mask overload and lead to crashes afterwards.
So again, the aim should not be to simply add more strategies to the client’s toolkit. It is to create the conditions where communication support feels collaborative, sustainable and less dependent on pressure, masking or over-effort.
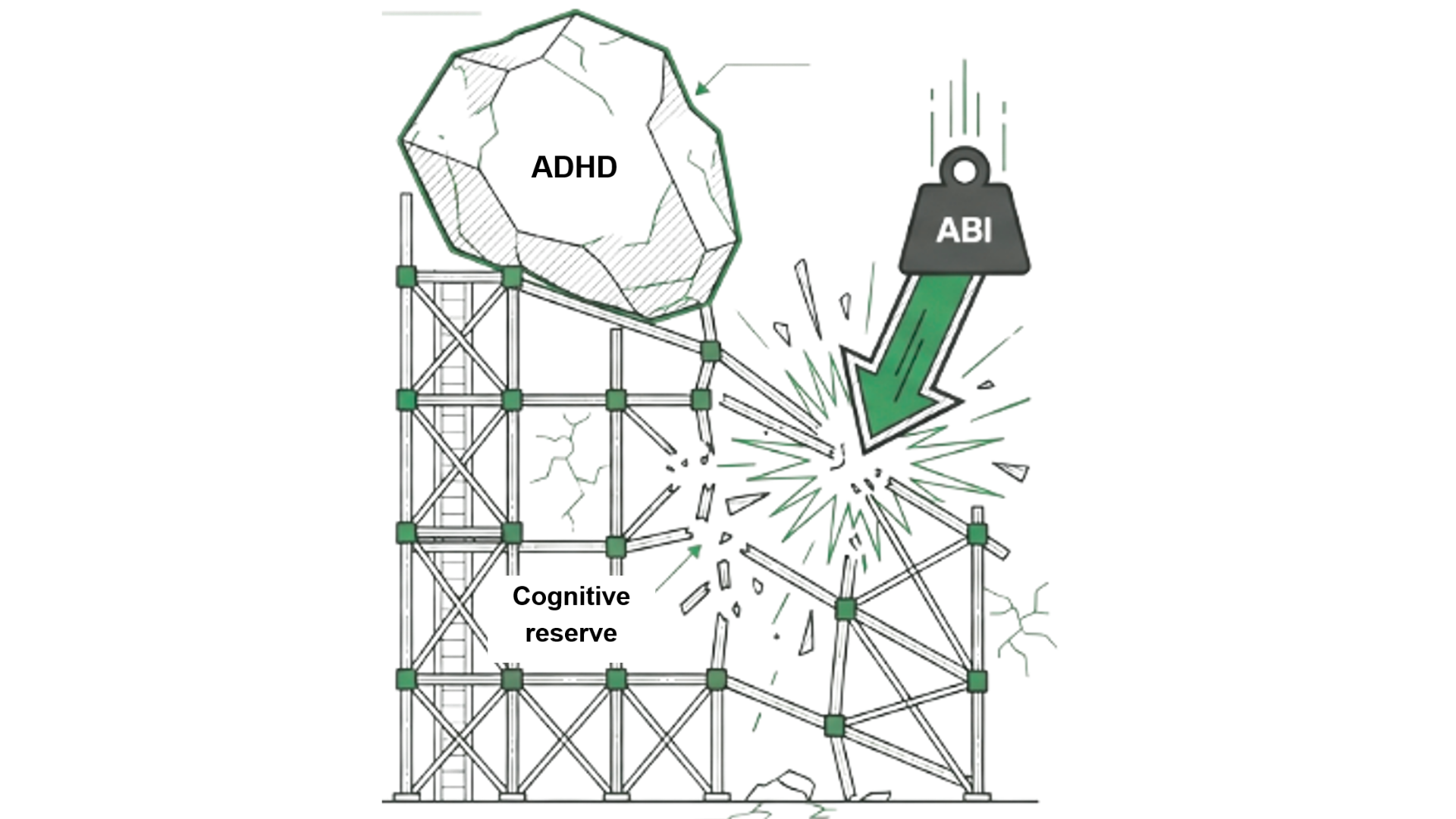
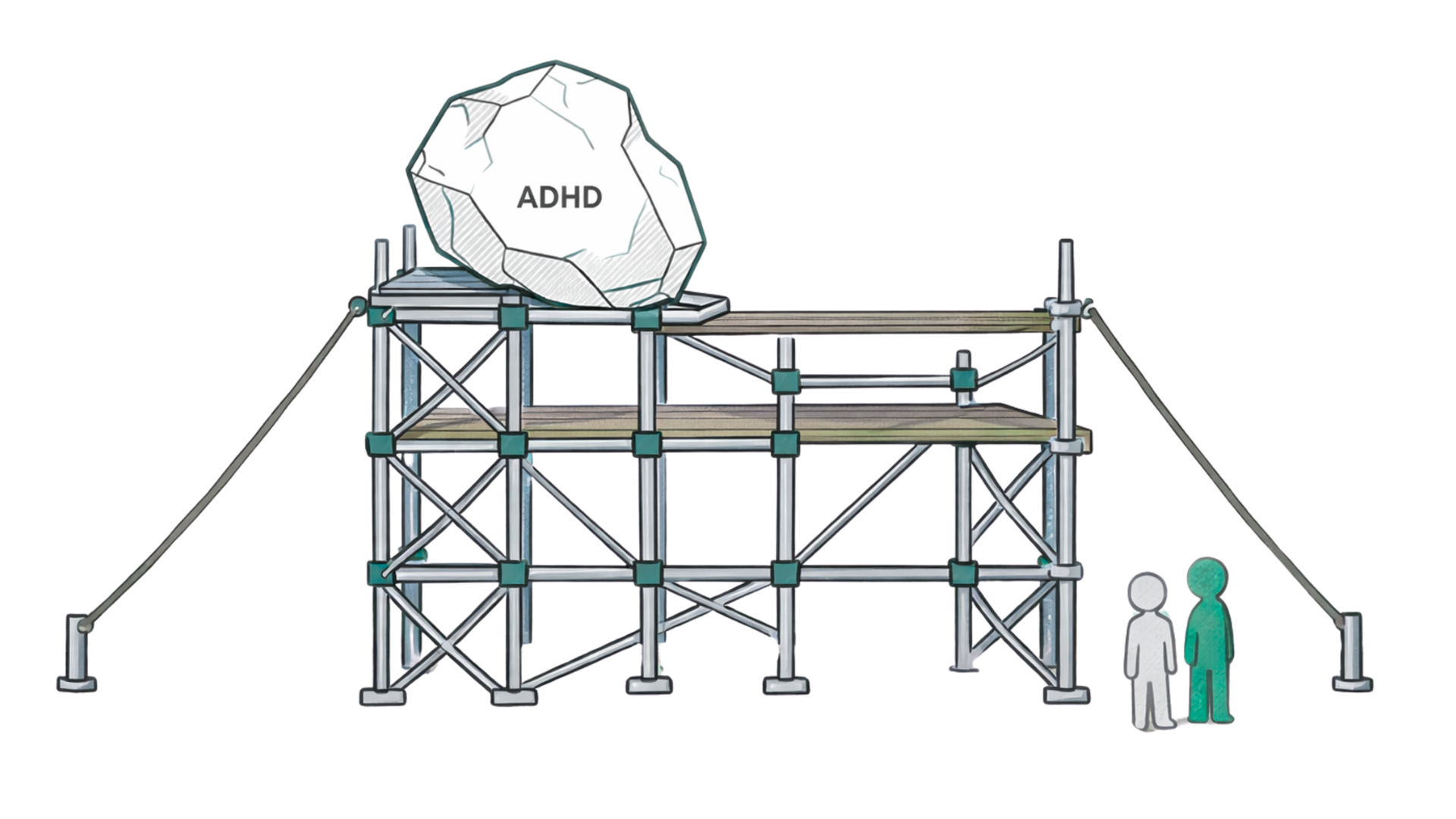
The scaffold - from individual coping to shared responsibility
For some adults with ADHD, life before ABI may already have involved a complex scaffold of coping strategies: urgency, over-preparation, anxiety-driven performance, masking, external systems, self-monitoring, support from others, or simply pushing through.
These strategies may have worked well enough before the injury, even if they came at a cost.
After ABI, that same scaffold may no longer be accessible.
Reduced cognitive reserve, fatigue, emotional changes, sensory load and new cognitive-communication difficulties can make old ways of coping less sustainable.
The person may not only be adjusting to the effects of brain injury, but also to the loss of the strategies that previously helped them manage, compensate or appear “fine”.
This is why ADHD-informed ABI rehabilitation should not simply be about adding more strategies.
It is about building a different kind of scaffold: one that distributes the load more sustainably across the person, their environment, communication partners, routines, values, strengths, supports and rehabilitation team.
Building a new, more sustainable scaffold
This might mean fewer internal and external demands, more environmental support, more communication partner adaptation, clearer shared expectations, more self-advocacy, better pacing and regulation, less reliance on masking, and promoting more self-compassion.
This shifts the focus away from the client having to keep working harder internally, and towards building a system around them that makes communication less effortful and more sustainable.
That scaffold is likely to be strongest when therapy is neurodiversity-affirming, trauma-informed, values-aligned, strengths-based and collaborative.
When we keep shame, autonomy, capacity and the therapeutic relationship in mind, we are more likely to create communication support that is not only clinically effective, but usable in real life.
Want to explore this in more depth?
This article gives a top-level overview of ADHD and ABI communication rehabilitation. In my 80-minute recorded webinar, I explore these ideas in more clinical depth, including the reasoning, evidence and implications for SLT practice.
The main focus of the webinar is on how to apply this clinically. I introduce the TalkCoach 5 Pillar Framework for ADHD Communication, a practical framework for thinking about ADHD-informed communication support in ABI rehabilitation.
The webinar includes some examples and clinical ideas for adapting assessment, formulation, feedback, home practice, goal-setting and therapy tasks in ways that are neurodiversity-affirming, trauma-informed and realistic for everyday clinical work.
The webinar is designed for Speech and Language Therapists and rehabilitation professionals working with adults with ABI, cognitive-communication difficulties, ADHD and/or complex neurodivergent profiles.
It includes:
an 80-minute recorded webinar
accompanying slides
the TalkCoach 5 Pillar Framework for ADHD Communication
practical examples and ideas for applying the framework in clinical practice
Looking to refer a client?
At TalkCoach, we support adults with acquired brain injury, ADHD and other neurological conditions.
We work with clients, families, case managers and rehabilitation teams to support communication in a way that is practical, person-centred and neurodiversity-affirming.
Find out more about ourSpeech and Language Therapy services.
If you would like to discuss a referral, please get in touch.
Reference
Ilie, G., Vingilis, E. R., Mann, R. E., Hamilton, H., Toplak, M., Adlaf, E. M., Kolla, N., Ialomiteanu, A., van der Mass, M., Asbridge, M., Vingilis-Jaremko, L., Rehm, J., & Cusimano, M. D. (2015). The association between traumatic brain injury and ADHD in a Canadian adult sample. Journal of Psychiatric Research, 69, 174–179.